


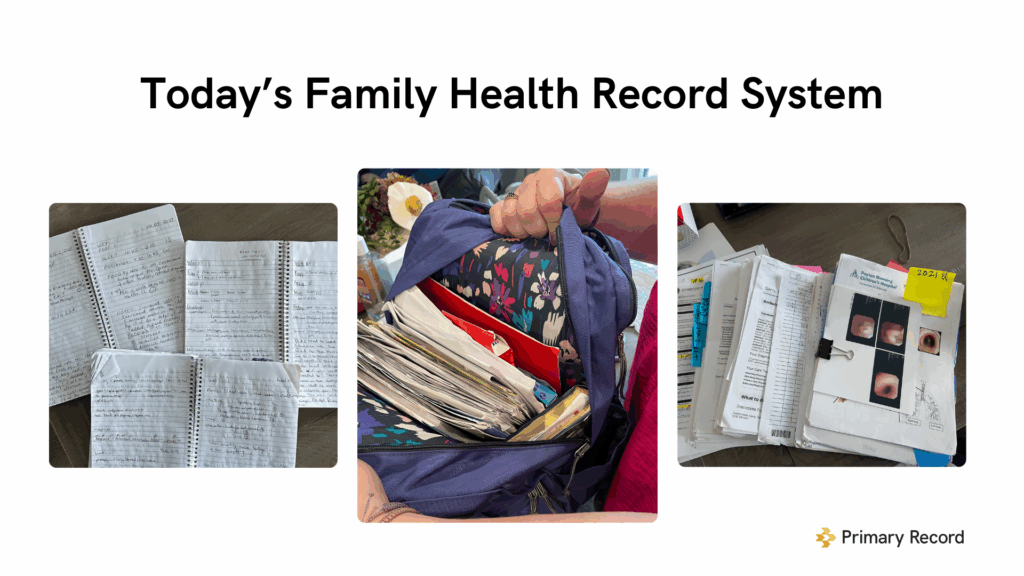
In every home I’ve ever visited as a nurse care coordinator from rural Indiana to crowded city apartments, I’ve seen the same thing: a kitchen table covered in paperwork, a binder full of printouts, and a family member trying to make sense of disconnected medical information
For families, this is interoperability.
That reality is what inspired Primary Record and what ultimately helped a small startup from Indiana win the 2025 AMIA FHIR App Competition. Our focus has always been the same: bring the power of FHIR to where health actually happens… the home.
Now, heading into 2026, momentum is growing. Federal enforcement is strengthening, states are redesigning community care, and families are demanding more than access; they want tools that make their care easier to understand and follow.
This page explores why patient-directed interoperability matters, how FHIR helps, what stands in the way, and why a new generation of tools is emerging to deliver the last mile of care coordination.
What Is Patient-Directed Interoperability?
Most interoperability efforts focus on provider-to-provider exchange, the movement of data across hospitals, clinics, payers, and labs.
But increasingly, the people who coordinate the most care are not inside those systems:
- family caregivers,
- community paramedics,
- school nurses,
- senior living nurses,
- advocates,
- home health teams.
Patient-directed interoperability shifts the center of gravity. It enables patients and their designated caregivers to gather, manage, and share their health information across systems, across settings, and across time.
Why it matters now
- Families manage more chronic illness than ever.
- Care is increasingly delivered in the home.
- Patients see multiple providers across disconnected systems.
- New federal models (ACCESS, RHTP) will require (and pay for!) community coordination.
- AI tools depend on complete, longitudinal record inputs.
In today’s healthcare landscape, the home has become a clinical environment, but the data infrastructure hasn’t followed.
The Real Problem: Interoperability Breaks Where Life Happens
Inside the health system, data flows.
Outside the health system, where families coordinate medications, appointments, benefits, and daily living, everything breaks down.
Families still rely on:
- phone
- binders
- notebooks
- Google Drive folders
- screenshots
- printed portal pages
Meanwhile, community-based teams are disconnected:
- Paramedics manually copy/paste EHR data out and into their system
- Senior living nurses “hunt down” discharge summaries
- School nurses re-enter data into non-integrated systems
- Home health teams are denied access or rely on fax
These people provide critical care.
But they operate outside the data ecosystem.
FHIR has given us the first real standard that lets patients and families interact with the healthcare system, and in doing so, creates a path to connect communities through the patient, not the institution.
FHIR: What It Enables And What It Doesn’t
FHIR has been transformational for getting data into consumers’ hands. Using the FHIR R4 Patient Access APIs, families can retrieve on Primary Record today:
- medications
- labs
- allergies
- conditions
- vaccinations
- visits
- procedures
This is powerful.
But real care coordination requires more than access.
Families and caregivers need:
- reliability
- provenance
- context
- shared authority
- workflows
….and a way to fill the gaps when data is missing
Key missing pieces in today’s patient access APIs
From real-world experience:
- APIs break silently, with no alert to the patient (or the consumer app!)
- Data available in portals does not always appear in the apps families use to bring multiple systems together
- Identity models assume individual autonomy, not shared caregiving
- No enforcement (yet) when there are barriers to getting information electronically
For patients and families, this means they may believe they’re accessing a full record… when in reality, they’re not. And if we want FHIR to scale into the community, this becomes a major hurdle because this experience breaks trust.
And trust is the key to interoperability.
Not just for sharing data outside covered entities, but for getting patients, their caregivers, and community supports to engage, participate, and continue using FHIR-powered tools in their daily lives to improve health.
Why the Last Mile Matters: Homes Are Mini-Hospitals
When you walk into the home of a complex patient, what some of you who have never lived it would see:
- oxygen equipment
- dialysis schedules
- visiting nurses
- PT/OT notes
- medication changes
- symptom logs
- family group texts
- care calendars
- benefit and insurance letters
It is a clinical environment without a clinical infrastructure.
Health systems may perform the surgery.
But, families perform the recovery.
They coordinate 90% of care that happens between encounters, and they do it from “systems” that look like this:
Patient-directed interoperability ensures data can reach:
- the caregiver who will be changing a wound
- the school nurse who may be administering medications
- the senior living nurse creating a fall risk plan
- the paramedic treating a resident in the field
This is the real-world value of FHIR.
The Four Barriers Standing in the Way
Based on thousands of hours poured into building and gaining traction with Primary Record, these are our systemic blockers:
1. API Reliability & Data Quality
Families expect what they see in their portal to match what they see in an app.
It often doesn’t.
APIs must be treated as safety infrastructure, not optional add-ons.
2. Identity & Consent Don’t Reflect Shared Care
Care is shared.
Portal access is not.
Today, many families resort to sharing passwords, a symptom of a broken consent model.
3. Access Alone Doesn’t Create Coordination
We must move away from the idea of someone needing a personal health record (PHR). They imply a passivity that does not match the patient and caregiver experience.
Caregiving is active work: medication reconciliation, symptom tracking, updating family members, home care teams, and managing forms.
Families need coordination systems, not viewable document storage.
4. Economics Don’t Support the Last Mile
The people who do the most coordination, families, social workers, community paramedics, senior living nurses, are the least funded.
Digital care coordination isn’t reimbursed.
Until that changes, true scale is impossible.
Four Forces Driving Change in 2026
Despite these barriers, we are entering a once-in-a-generation moment of alignment.
1. Federal Enforcement Is Strengthening (OIG + ASTP)
Information blocking enforcement is becoming real.
Families should not have to fax for records in 2026.
Federal leaders are listening, and they want our stories.
2. States Are Preparing for a 2026 Interoperability Shift Around Rural Health & Primary Care
The CMS ACCESS Model and Rural Health Transformation Program are pushing states to support consumer-facing data tools and community care coordination models.
3. CMS’s Health Tech Ecosystem Is Opening Doors
Primary Record pledged to “kill the clipboard” and use conversational AI to strengthen communities.
CMS is signaling clear support for consumer-centered innovation.
4. Community Businesses and Care Teams Are Showing the Way Forward
The real blueprint for patient-directed interoperability isn’t coming from large institutions; it’s coming from the community.
Our community partners in care management and advocacy are showing what it actually takes to onboard families, build trust, and sustain engagement. They are the ones walking into homes, sitting at kitchen tables, and helping families manage the daily realities of care.
These teams are proving the demand.
When families are supported, when someone helps them connect portals, interpret data, invite caregivers, and integrate information into daily routines, engagement rises dramatically.
Families using Primary Record are demonstrating a simple truth:
Consumer need is undeniable.
Community readiness is here.
And the market timing has arrived.
The Future: What Patient-Directed Interoperability Can Make Possible
Imagine a world where:
- APIs never break silently
- Caregivers have permissioned, delegated authority
- Every discharge packet flows automatically to the family
- School nurses receive updated action plans instantly
- Paramedics have access to meds, allergies, and care plans in the field
- Families coordinate confidently instead of chaotically
- AI tools generate insights from a complete longitudinal record
This is what FHIR makes possible.
This is what policy must support.
This is what families deserve.
Conclusion: The Solution Starts With You
The problem is big.
It’s tangled.
It spans technology, policy, and human egos & experience.
But the movement starts small:
Solve it for yourself.
Solve it for your family.
Solve it for your neighbor and community.
If we commit to improving the flow of information at the human level at the kitchen table, we can build a world where health information is 100% available whenever and wherever it’s needed.
That is the future Primary Record is committed to building.


